Most people think of COPD as something that comes from smoking. But what if your lungs are failing even though you never lit a cigarette? For some, the real cause is a hidden genetic flaw called Alpha-1 Antitrypsin Deficiency - or AATD. It’s not rare. It’s just overlooked.
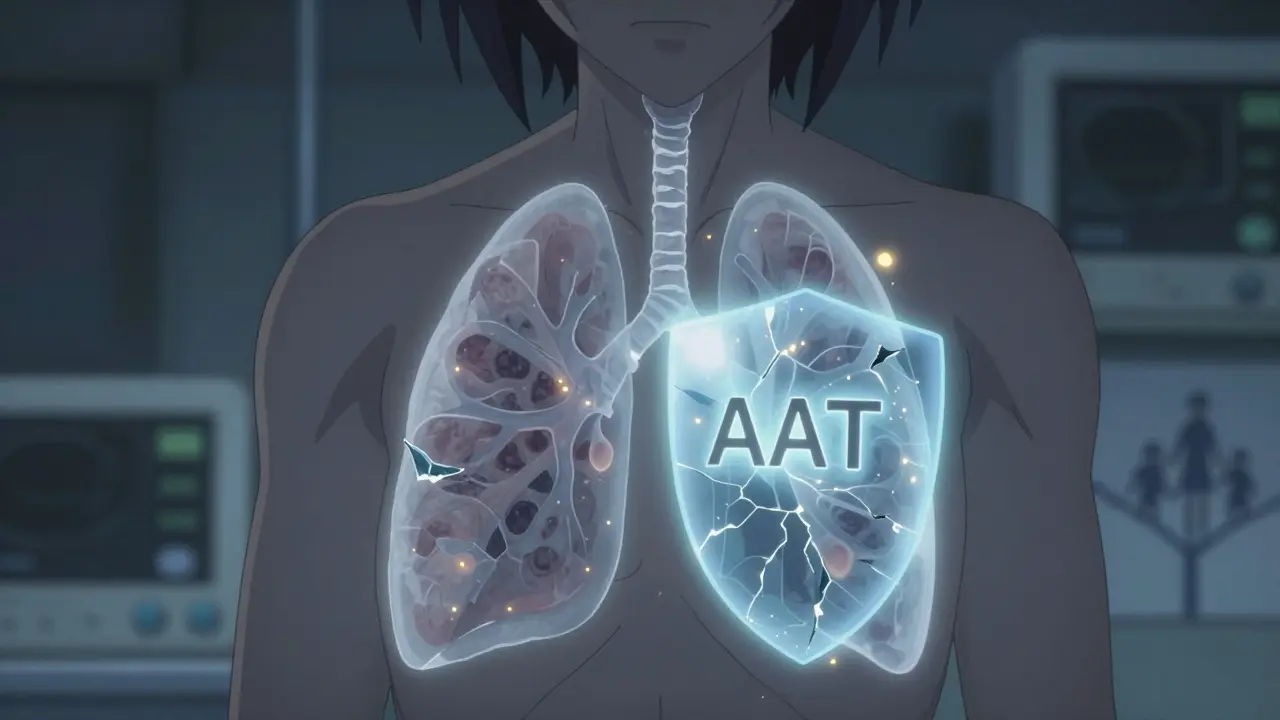
Imagine your lungs have a built-in shield. That shield is a protein called alpha-1 antitrypsin (AAT). It stops white blood cells from tearing apart lung tissue. When AAT is missing or broken, those cells go unchecked. Over time, the air sacs in your lungs get destroyed. That’s emphysema. And it can start as early as your 30s. This isn’t just bad luck - it’s in your genes.
What Exactly Is AATD?
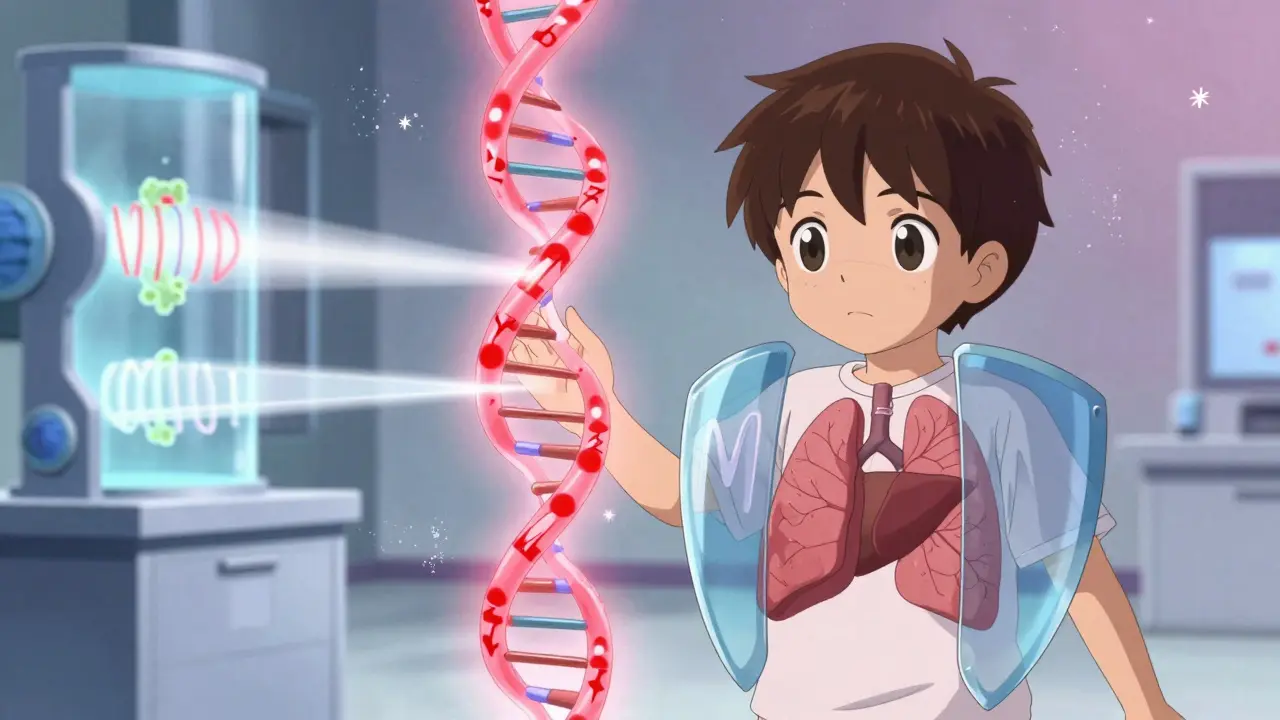
AATD is caused by mutations in the SERPINA1 gene a gene on chromosome 14 that makes the alpha-1 antitrypsin protein. Everyone inherits two copies - one from each parent. If both copies are faulty, you’re at highest risk. The most common bad version is called the Z allele. If you have two Z alleles (PiZZ genotype), your body makes only 15-20% of the AAT you need. That’s not enough to protect your lungs.
Normal AAT levels sit between 100 and 200 mg/dL. People with PiZZ often have levels as low as 11-17 mg/dL. That’s why lung damage starts so young. Most people with smoking-related COPD don’t see symptoms until after 60. AATD patients? Often by 40. And it’s not just the lungs. The liver makes AAT. When the protein folds wrong - like in the Z variant - it piles up inside liver cells. That can lead to cirrhosis, liver failure, or even liver cancer. About 10-15% of adults with PiZZ develop serious liver disease.
Why Is It So Hard to Diagnose?
Here’s the problem: AATD looks exactly like asthma or regular COPD. Chronic cough. Wheezing. Shortness of breath. Doctors treat the symptoms. They don’t look for the root cause.
Studies show it takes an average of eight years and three different doctors before someone with AATD gets the right diagnosis. Many are told they have "chronic bronchitis" or "refractory asthma." Some even get inhalers for years before anyone tests their AAT levels.
The American Thoracic Society and European Respiratory Society say: test everyone with COPD. Test anyone under 45 with unexplained emphysema. Test people with liver disease of unknown cause. But only about 10% of those who should be tested actually are. In the U.S., an estimated 100,000 people have severe AATD. Only 10,000 know it.
How Is It Tested?
It starts with a simple blood test. Your doctor checks your serum AAT level. If it’s below 11 μM (about 50 mg/dL), they’ll do a follow-up test: genotyping or phenotyping.
- Genotyping looks for specific mutations - like Z or S - in your DNA.
- Phenotyping uses a lab technique called isoelectric focusing to see what shape the protein takes. It’s more precise but slower and less available.
Once you know your genotype, you know your risk. PiMM? Normal. PiMZ? Mild risk. PiZZ? High risk for lung and liver damage. PiSZ? Moderate to high risk. Even if you’re a carrier - like PiMZ - smoking can push you into disease territory. That’s why quitting is non-negotiable.
Smoking Changes Everything
Let’s be clear: if you have AATD and you smoke, you’re playing Russian roulette with your lungs. Studies show smoking cuts the age of emphysema onset by 10-15 years. One patient, diagnosed at 42, stopped smoking and said it likely added 15+ years to his life. That’s not hype - it’s science.
Even if you don’t smoke, secondhand smoke, pollution, or dust can speed up damage. That’s why avoiding lung irritants is as important as any treatment.
Treatment: Augmentation Therapy
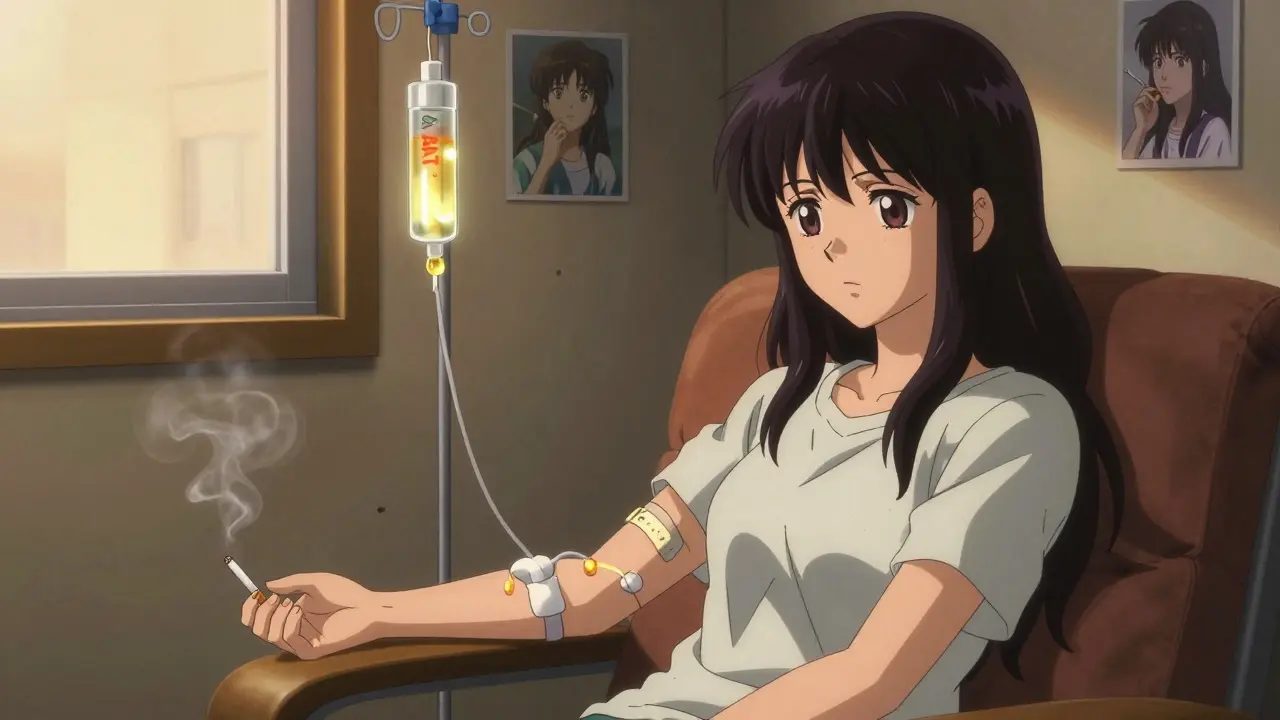
There’s no cure. But there is a treatment that replaces what your body can’t make: augmentation therapy intravenous infusions of purified human alpha-1 antitrypsin protein.
You get a weekly IV drip of AAT - usually 60 mg per kilogram of body weight. The goal? Keep your blood levels above 11 μM. That’s the minimum level shown in labs to stop lung destruction.
Three FDA-approved products are used in the U.S.: Prolastin-C (Takeda), Zemaira (CSL Behring), and Aralast NP (Grifols). They all work the same way. The difference? Cost and availability.
Each year, this therapy costs $70,000-$100,000. Insurance often denies the first claim. You’ll need your doctor to appeal. Many patients spend months fighting for approval. And even when approved, you’re stuck with a 2-hour weekly infusion. Some people can’t find veins. Others can’t take time off work. It’s a heavy burden.
But here’s the upside: studies show augmentation therapy slows lung function decline by 30-50% compared to no treatment. It doesn’t reverse damage. But it can keep you breathing longer.
What About the Liver?
Augmentation therapy doesn’t help the liver. The problem there isn’t low AAT - it’s the bad protein clogging up liver cells. Right now, there’s no drug to fix that. The only option for advanced liver disease is a transplant.
That’s why researchers are racing to develop new therapies. One approach? Small molecules that stop the Z protein from clumping. Another? Gene therapy to replace the faulty SERPINA1 gene. Early trials are showing promise. A Phase II trial using RNA interference (NCT04735716) aims to silence the mutant gene in the liver - basically turning off the bad version.
And in 2022, the FDA approved the first subcutaneous AAT treatment - Kedrab - which you can inject yourself at home. It’s not yet widely available, but it’s a step toward less invasive care.
Who Should Get Tested?
You should consider testing if:
- You were diagnosed with COPD before age 45
- You have emphysema without a smoking history
- You have unexplained liver disease
- You have a family member with AATD
- You have asthma with fixed airflow obstruction
Even if you’re not symptomatic, knowing your status matters. If you’re a carrier (PiMZ), your kids might inherit the Z allele. Genetic counseling can help you understand the risks.
The Bigger Picture
AATD is a wake-up call. It proves that not all COPD is lifestyle-related. Genetics matter. And when we miss it, we miss a chance to act early.
Right now, only 12 U.S. states screen newborns for AATD. That’s changing. Experts argue that early detection could prevent decades of suffering. Imagine knowing at birth you carry the Z allele. You grow up avoiding smoke. You get regular lung checks. You start therapy before damage begins. That’s not science fiction - it’s the future we’re building.
The cost of treatment is high. But the cost of not treating? Lung transplants. Liver failure. Lost years. Lost jobs. Lost life.
For those with AATD, this isn’t just about managing a disease. It’s about reclaiming time. And time - more than anything - is what they fight for.
Can you outgrow Alpha-1 Antitrypsin Deficiency?
No. AATD is a lifelong genetic condition. You’re born with it. You can’t outgrow it. But you can manage it. Early diagnosis, avoiding smoking, and starting augmentation therapy when appropriate can slow progression and improve quality of life. The gene doesn’t change - but your choices do.
Is AATD only a lung disease?
No. While lung damage is the most common symptom, AATD also affects the liver. The faulty protein builds up in liver cells, causing inflammation, scarring, and sometimes cirrhosis or liver cancer. Some people develop liver problems before any lung symptoms appear. That’s why testing both organs is critical.
Can I pass AATD to my children?
Yes. AATD is inherited in an autosomal codominant pattern. If you have one faulty copy (like PiMZ), each child has a 50% chance of inheriting it. If both parents carry a faulty gene, children could end up with two bad copies (PiZZ) - which carries the highest risk. Genetic counseling before having children can help assess risks and plan testing.
Does augmentation therapy stop emphysema completely?
No. It doesn’t reverse existing damage. But it can slow the rate of lung function decline by 30-50%. Think of it like putting a shield on a rusting car - it won’t fix the rust, but it stops more from forming. Starting therapy early, before major damage occurs, gives the best results.
Why isn’t everyone tested for AATD?
Because it’s still underrecognized. Many doctors aren’t trained to think of it. Testing isn’t routine. And the cost of treatment is high, so insurers often push back. But guidelines from the American Thoracic Society and European Respiratory Society clearly recommend testing all COPD patients. The gap between recommendation and practice is huge - and it’s costing lives.
Are there new treatments on the horizon?
Yes. Several are in clinical trials. RNA interference therapies aim to silence the faulty gene in the liver. Small molecule correctors help the protein fold properly. Gene therapy and CRISPR-based edits are being tested too. The first subcutaneous AAT product (Kedrab) is already approved. These aren’t just improvements - they’re potential game-changers for liver disease and treatment burden.
For someone with AATD, the path isn’t easy. But it’s not hopeless. The tools exist. The knowledge is there. What’s missing is awareness. And that’s changing - one test, one diagnosis, one life at a time.
Joe Grushkin
February 15, 2026 AT 22:04Virginia Kimball
February 17, 2026 AT 09:45Chiruvella Pardha Krishna
February 19, 2026 AT 06:23Sarah Barrett
February 19, 2026 AT 12:55Kaye Alcaraz
February 20, 2026 AT 14:25Erica Banatao Darilag
February 21, 2026 AT 15:27Charlotte Dacre
February 23, 2026 AT 06:01Esha Pathak
February 24, 2026 AT 09:57