When someone is diagnosed with osteoporosis, the big question isn't just what treatment to start-it's whether it's working. Waiting a full year or two to see if bone density improves on a DXA scan feels like driving blindfolded. That’s where bone turnover markers (BTMs) come in. These are simple blood or urine tests that show how fast your bones are breaking down and rebuilding. And unlike DXA scans, they give you answers in weeks, not years.
What Are Bone Turnover Markers?
Bone is never still. Every day, old bone is removed by cells called osteoclasts, and new bone is built by osteoblasts. This process is called remodeling. Bone turnover markers are tiny fragments and enzymes released during this process. Some come from bone breakdown (resorption), others from bone building (formation). Measuring them gives a real-time snapshot of what’s happening inside your skeleton.
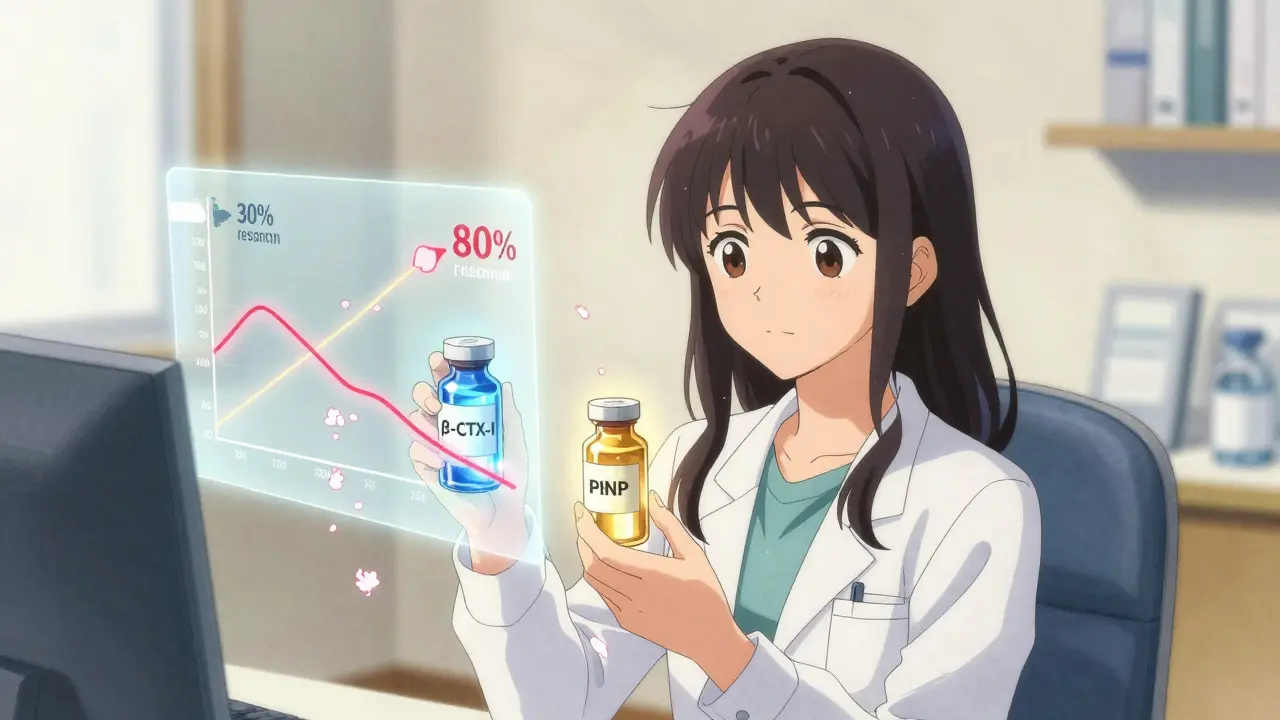
Not all markers are created equal. The International Osteoporosis Foundation and European Calcified Tissue Society agree on two as the gold standards: serum PINP (procollagen type I N-terminal propeptide) for bone formation, and plasma β-CTX-I (beta-C-terminal telopeptide of type I collagen) for bone resorption. These two are the most reliable, with the least interference from diet, time of day, or lab methods.
Why Use Them Instead of Just a DXA Scan?
DXA scans measure bone mineral density (BMD). They’re great for diagnosis and tracking long-term changes. But here’s the catch: it takes 12 to 24 months to see a meaningful change in BMD, even if the drug is working perfectly. That’s a long time to wait, especially if you’re worried the medication isn’t helping-or if you’ve missed doses.
BTMs change much faster. Within 3 to 6 weeks of starting treatment, you’ll see a shift. For example, if you begin a bisphosphonate like alendronate (an anti-resorptive drug), β-CTX-I levels drop by 30% or more within 3 months. If they don’t, it’s a red flag. Maybe you’re not taking the pill. Maybe your body isn’t responding. Maybe you need a different drug.
For anabolic treatments like teriparatide, the story flips. PINP levels jump 70% to 100% within 1 to 3 months. That’s a clear signal the bone-building machinery is turning on.
A 2022 study called TRIO showed patients who had a 30% drop in β-CTX-I at 3 months had a 1.6% lower fracture risk after just 22 weeks. That’s a real-world benefit-not a lab curiosity.
How Are They Measured? What You Need to Know
These aren’t routine blood tests. There are strict rules to get accurate results.
For β-CTX-I (resorption marker):
- Must be drawn in the morning, between 8 and 10 a.m.
- Requires overnight fasting (no food or drink except water after midnight)
- Should be done before taking any osteoporosis meds that day
- Post-meal levels can spike by 20-30%, ruining accuracy
For PINP (formation marker):
- Less affected by meals or time of day
- Still best to collect in the morning
- No fasting needed
Lab methods matter too. Automated immunoassays are now standard. Older methods like radioimmunoassays (RIA) are fading out. Accuracy depends on using the same lab and test method each time-switching labs can give false readings.
The least significant change (LSC) is the smallest drop or rise that means something real. For β-CTX-I, it’s 25%. For PINP, it’s 20%. If your level changes less than that, it’s probably noise-not a treatment effect.
Who Should Get Tested?
BTMs aren’t for everyone. They’re most useful in three situations:
- Starting treatment: Get a baseline before you begin any osteoporosis drug. This gives you a reference point.
- 3 months after starting: Check again. Did PINP go up (if on teriparatide)? Did β-CTX-I go down (if on a bisphosphonate)? If not, talk to your doctor. You might need to adjust your dose, switch drugs, or check for adherence.
- When adherence is questionable: If you’ve missed pills, skipped injections, or stopped treatment, BTMs can show whether your bone turnover is still high-meaning you’re still at risk.
They’re also helpful for people with kidney disease. In chronic kidney disease (CKD), traditional markers like PINP and β-CTX-I can be misleading because the kidneys can’t clear them properly. In those cases, bone alkaline phosphatase (BALP) or TRACP5b are better options.
Limitations and What They Can’t Do
BTMs are powerful, but they’re not magic.
They don’t tell you where the bone is changing. A drop in β-CTX-I doesn’t mean your spine is getting stronger-it just means overall bone breakdown is slowing. That’s why DXA scans are still needed. BTMs and DXA work together.
They’re also noisy. Biological variability can be high-up to 60% in some cases. That’s why you need two measurements: baseline and follow-up. One test alone means nothing.
And they’re not perfect for everyone. Reference ranges are mostly based on Caucasian populations. Asian women often have 15-20% lower baseline β-CTX-I levels. African populations show higher PINP. Labs are working to fix this, but it’s not standardized yet.

What If the Numbers Don’t Change?
If your β-CTX-I didn’t drop 30% after 3 months on a bisphosphonate, you’re not alone. About 1 in 4 people are non-responders. It could be:
- You’re not taking the pill correctly
- You have low vitamin D or calcium
- You have secondary causes of bone loss (like thyroid disease or steroids)
- Your body just doesn’t respond to that drug
That’s when BTMs shine. Instead of waiting a year to see if you fracture, you catch the problem early. Your doctor can switch you to a different drug-like denosumab or romosozumab-before it’s too late.
One study found BTM monitoring identified non-adherent patients with 85% accuracy. That’s huge. It means you’re not just guessing whether someone is taking their meds-you’re seeing the biological truth.
The Future of BTMs
More guidelines are coming. The American Association of Clinical Endocrinologists plans to update its osteoporosis recommendations in mid-2024 to include BTMs as standard practice. Medicare already covers PINP and β-CTX-I testing with CPT codes 83970 and 83935. Reimbursement is around $30 per test.
Point-of-care tests are in development. Imagine a simple finger-prick test in your doctor’s office that gives results in 15 minutes. That’s the next frontier.
And research is expanding. Clinical trials are now looking at whether BTMs can predict fracture risk better than BMD alone. Others are studying how to personalize treatment-using BTMs to tell you exactly when to stop or switch drugs.
Bottom Line
Bone turnover markers aren’t replacing DXA scans. They’re making them smarter. If you’re on osteoporosis medication, ask your doctor about checking PINP and β-CTX-I at 3 months. It’s a fast, low-risk way to know if your treatment is working. No waiting. No guesswork. Just clear, objective data that helps you stay strong-and avoid fractures before they happen.
Are bone turnover markers better than DXA scans for monitoring osteoporosis?
No, they’re not better-they’re different. DXA scans measure bone density and are the gold standard for diagnosis and long-term tracking. But they take 1-2 years to show changes. Bone turnover markers show how fast your bones are remodeling and can show treatment effects in 3-6 weeks. They work best together: use BTMs for early feedback, DXA for final confirmation.
Can I use bone turnover markers to diagnose osteoporosis?
No. Bone turnover markers cannot diagnose osteoporosis. Diagnosis requires a DXA scan that shows low bone mineral density. BTMs only tell you how active your bone remodeling is-not how dense your bones are. They’re used to monitor treatment after diagnosis, not to make the initial call.
Do I need to fast before a bone turnover marker test?
It depends on which marker is being tested. For β-CTX-I (the resorption marker), yes-you must fast overnight and have the blood drawn between 8 and 10 a.m. Food and time of day can throw off results by 20-40%. For PINP (the formation marker), fasting isn’t required, but morning collection is still recommended for consistency.
Why do some people not respond to osteoporosis drugs?
There are several reasons. Poor adherence (missing doses) is the most common. Others include low vitamin D or calcium, kidney disease, thyroid problems, or genetic factors. Some people simply don’t respond to certain drugs. Bone turnover markers help catch this early-before fractures occur-so your doctor can switch to a more effective treatment.
How often should bone turnover markers be checked?
For most people starting osteoporosis treatment, check once before starting, then again at 3 months. If the response is good, further testing isn’t usually needed until the next DXA scan at 12-24 months. If there’s no response, repeat testing at 6 months may help guide a change in therapy. Routine annual testing isn’t recommended unless there’s a reason to suspect non-adherence or treatment failure.
Are bone turnover marker tests covered by insurance?
Yes, in the U.S., Medicare covers both PINP (CPT 83970) and β-CTX-I (CPT 83935) for monitoring osteoporosis therapy. Private insurers vary, but coverage is improving as guidelines update. Check with your provider, but many now approve these tests when ordered for treatment monitoring after diagnosis.
Cory L
February 23, 2026 AT 19:40Whoa, this is game-changing. I’ve been on alendronate for 8 months and was totally in the dark. Found out my β-CTX-I dropped 40% at 3 months - felt like my bones were finally waking up. No more guessing. Just science. Love it.
Lisandra Lautert
February 25, 2026 AT 13:41Bone turnover markers aren't just useful-they're essential.
Jacob Carthy
February 26, 2026 AT 20:28Why are we even talking about this like it's some new miracle? We've had these tests for over a decade. The real problem? Doctors don't order them. And insurance? Half the time they won't cover it unless you beg. This isn't innovation-it's neglect wrapped in a lab report.
kirti juneja
February 27, 2026 AT 04:49As someone from India, I’ve seen how expensive these tests are. My mom’s doctor didn’t even mention BTMs until she had two fractures. We paid out of pocket. But once we got the numbers? Total game-changer. Switched from bisphosphonate to denosumab. No more scary falls. You don’t need fancy gear-just someone who cares enough to ask for the test.
Larry Zerpa
February 28, 2026 AT 20:03Let’s be real: this whole BTM hype is just Big Pharma’s way of selling more tests. You think your doctor really cares if your PINP went up 70%? No. They care if you paid for the follow-up. And let’s not forget: these markers fluctuate like a stock market ticker. One bad coffee, one late night, and your numbers are garbage. This isn’t precision medicine-it’s placebo science with a price tag.
tia novialiswati
March 1, 2026 AT 07:32This is so validating 💪 I was scared to start treatment because I thought I’d be stuck waiting a year to know if it worked. Now I know: if my β-CTX-I drops, I’m on the right path. And if it doesn’t? I’ll speak up. Thank you for making this feel doable.
Bhaskar Anand
March 2, 2026 AT 11:35USA thinks it owns medical science but forgets that India has been using bone markers for decades in rural clinics with basic equipment. We don’t need fancy immunoassays. We need access. Your CPT codes won’t help a farmer in Bihar whose spine is collapsing. Real medicine isn’t about codes-it’s about reaching people.
Shalini Gautam
March 3, 2026 AT 00:27I got my first BTM test after my hip fracture. My doctor said it was "experimental." I paid $180 out of pocket. My β-CTX-I was through the roof. Turned out I’d been skipping my pills because I thought they made me nauseous. Turns out I just wasn’t taking them right. This test saved me from another fracture. Don’t let anyone tell you it’s not worth it.
William James
March 3, 2026 AT 09:26I’m not a doctor but I’ve watched my dad go through this. The thing that hit me hardest? It’s not about the numbers-it’s about hope. Before BTMs, he felt like a time bomb. Now? He checks his levels like a weather report. If the wind’s shifting, he adjusts. It’s not magic. It’s agency. And that changes everything.
Brandice Valentino
March 4, 2026 AT 17:26Of course it works. I mean, obviously. But let’s be honest-this is just another way for elites to monetize aging. You think your average 70-year-old in rural Kansas knows what PINP is? Or that they can afford to fast until 10 a.m. and drive to a lab that even has the test? This isn’t progress. It’s exclusion dressed up as innovation.
Lillian Knezek
March 5, 2026 AT 00:33Wait… so they’re tracking bone turnover… but what if the government is using this to secretly monitor our bone density for future vaccine mandates? I read somewhere that the CDC has been collecting BTM data since 2019… and that’s when they started pushing osteoporosis meds… Coincidence? I think not. 🤔
Christopher Brown
March 5, 2026 AT 07:12BTMs are useless. Real doctors use DXA. Period. Anyone who says otherwise is either a researcher who’s never seen a patient or a lab tech trying to upsell. You want to know if your spine is strong? Get a scan. Not a blood draw. Not a urine cup. A scan. That’s medicine. The rest is noise.
Ashley Johnson
March 6, 2026 AT 02:36So if BTMs show improvement, does that mean I’m safe? Or is this just another lie? What if the lab is wrong? What if the machine is calibrated wrong? What if they’re hiding the real data? I’ve seen too many people get told they’re fine… then break a hip a month later. I’m not trusting this. Not one bit.